Gastric operations
Discuss the various gastric operations?
Distal/subtotal gastrectomy is performed for distal gastric cancers or peptic ulcer. Total gastrectomy (and Roux-en-Y anastomosis) is done for proximal gastric cancers.
The selection of an anastomosis method after a distal/subtotal gastrectomy is a highly debatable topic. Following subtotal gastrectomy, the intestinal continuity can be restored by:
- Billroth I
- Billroth II
- Roux-en-Y anastomosis
Billroth 1 is the preferred method of anastomosis in Japan. However, across Europe and North America, reconstruction using a Roux-en-Y anastomosis is more common. Functional results are better with Roux-en-Y anastomosis. Billroth II (vis a vis Billroth I) method of anastomosis was associated with higher rate of early postoperative complications
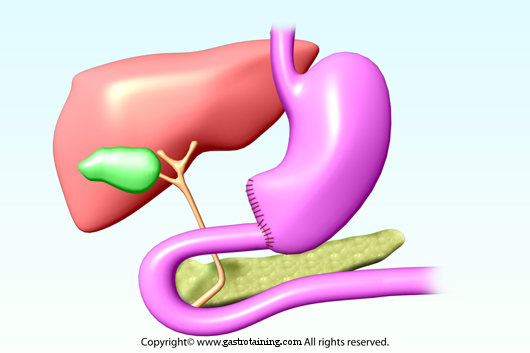
Billroth I- Stomach is directly anastomosed to duodenum
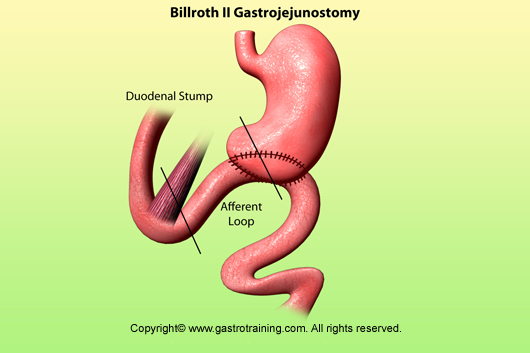
Billroth II- Jejunum is anastomosed to the stomach in a side to side manner (this creates a blind duodenal afferent loop)
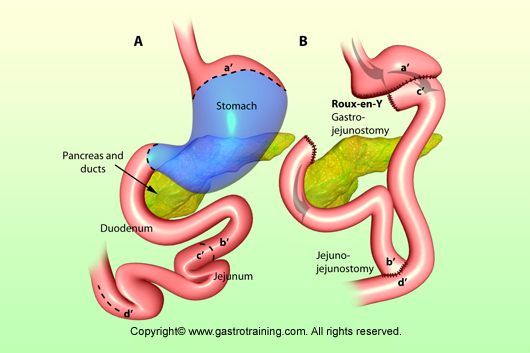
Roux-en-Y anastomosis- is done after total or subtotal gastrectomy. Jejunum is connected to the oesophagus or stomach. One end of the duodenum is sown up and the other end is connected to the jejunum (end to side anastomosis)
Polya gastrectomy- is a modification of Billroth II where full circumference of the open stomach is anastomosed to jejunum
Billroth I
Billroth II
Roux-en-Y-anastomosis